Bunion/Hallux Valgus
Diagnosis
Conservative treatment
As a first step in treatment, patients should try conservative measures prior to consulting with a surgeon.
-
Patients should be referred to a reputable orthopedic shoe store to obtain proper fitting supportive shoes with a wide toebox.
- Shoes that fasten with laces or buckles give the feet more support than slip-ons
-
They can also be given NSAIDs and/or Acetaminophen for pain
-
Custom orthotics
-
Toe spacers and/or Bunion guards
Surgical Treatment
Most patients do not need surgery. Surgery is done to relieve pain and not for cosmetic reasons.
There are several different surgical options for bunion surgery to achieve bony and soft tissue realignment. Arthrodesis is usually the treatment choice when arthritis has extensively damaged the joint.
Surgical correction of bunions is painful, and the recovery is long. It can take 6-12 months to fully recover and surgical patients will likely have to wear supportive shoes with a wide toebox for the rest of their lives.
Post-surgery, they may benefit from some physiotherapy treatment which will focus on helping the patient recover a normal gait pattern, foot biomechanics and function as well as mobility, strength and endurance
Diabetic Foot/Charcot Foot:
Diagnosis
- Clinical exam
- X-ray, MRI or bone scan of the foot
Management and Treatment
An acute infection, ulceration, or swollen, hot foot should be referred to the Emergency Department.
Chronic, stable Charcot Foot can be referred through Central Intake.
The
patient may be treated with a cast or a boot for about 3 months in
order to try to heal any fractures in the foot. In this case, the patient may have weight bearing restrictions, so they will need to use crutches, walker and/or a wheelchair. Once the swelling has decreased
and the bones are fused together, the patient will need a special custom
shoe.
Surgical treatment will depend on the deformity and the
patient condition but can involve debridement or procedures that include
replacement or fusions. Following surgery, patients will usually be
casted and will have weight-bearing restrictions on the foot for a
period of about 3 months.
Morton’s Neuroma
Diagnosis
- Clinical exam
- Diagnostic ultrasound or MRI may be considered if clinical testing is inconclusive, the patient has failed to respond to an initial course of conservative treatment and additional imaging is required to direct the course of treatment
Treatment
Conservative treatment
As a first step in treatment, patients should try conservative measures prior to consulting with a surgeon.
Conservative treatment includes:
- Wearing roomy shoes with a firm outer sole and low heel
- Cushioned orthotics
- Metatarsal pad in their shoes
- Over the counter anti-inflammatory or analgesic medication
- Local anesthetic or cortisone injection may be considered
- If you do not do cortisone / anesthetic injections, you can refer patients to a sports medicine physician
Cortisone will typically provide relief of symptoms for approximately 6 months. Normally, 80% of patients have less pain with these measures.
Surgical treatment
A small number of people require surgery. Most recover in a short period of time (6 – 8 weeks).
Hammer Toe
Diagnosis
Treatment
Conservative treatment
As a first step in treatment, patients should try conservative measures prior to consulting with a surgeon. Conservative treatment includes
- Roomy shoes with a broad toebox
- Physiotherapy to help address muscle strength and flexibility deficits
- Straps, cushions, or nonmedicated corn pads can be used to help align the toe and make it more comfortable
- Metatarsal pad
- Orthotics
A physiotherapist can help guide and prescribe an appropriate exercise program that may take into account any lower extremity issue contributing to the present problem.
Surgical Treatment
Failing conservative management, surgery can be performed to help with re-alignment and relieve the pain. The type of surgery and recovery will depend on the deformity.
Plantar Fasciitis
Diagnosis
X-rays are generally unnecessary however they may be useful to diagnose other conditions such as arthritis that do not respond to conservative treatment. Calcaneal bone spurs may be present but these do not necessarily correlate with symptoms.
Treatment
Conservative treatment
Conservative management is always the preferred management for pain from Plantar Fasciitis. Over 90% of patients get better with conservative treatment although it may take 6-18 months to recover.
This includes:
- Rest and activity modification
- Physiotherapy and exercises
- Ice and heat contrast (alternating 2 minutes of ice / 2 minutes of heat on the heel for a total of 12 to 16 minutes)
- NSAIDs and/or pain relievers
- Orthotics and supportive shoes
- Shockwave therapy
- Shockwave therapy is used to initiate a new healing response
Physiotherapy treatment should typically address pain relief, foot and gait analysis, exercises to strengthen intrinsic foot muscles and lower extremity/core, and education. Patients should beware of overstretching the structures as this may actually be a cause of the condition and/or perpetuate it.
Surgical treatment
Surgery is rarely considered. The type of surgery would depend on the patient’s presentation.
Arthritis
Diagnosis
Clinical exam and weight-bearing X-rays
Treatment
Conservative Treatment
As a first step in treatment, patients should try conservative measures prior to consulting with a surgeon.
Conservative management includes:
- Activity modification
- Physiotherapy
- Focus on activities and exercises that encourage mobility and improvements in strength and function
- Supportive footwear with a stiff rocker bottom sole
- Exercises that minimize stress on the joint (such as swimming or biking)
- Weight loss
- Walking aid (e.g.: cane, walking poles)
- cane is held in opposite hand from the painful foot
- Brace
- Orthotics
- NSAIDs or pain relievers
- Cortisone injection
- If you do not do cortisone injections, you can refer the patient to a sports medicine physician
Surgical treatment
Surgical management will depend on the joint affected and the degree of arthritis but can include arthroscopic debridement, joint replacement or fusion. After surgery, patients may need to have a cast or wear braces or special shoes for a period of time.Patients will often need to continue wearing adapted footwear such as a stiff-soled rocker shoe indefinitely.
Achilles Tendinitis/Tear
Diagnosis
- Clinical exam
- A complete Achilles tendon rupture is most often confirmed by executing a
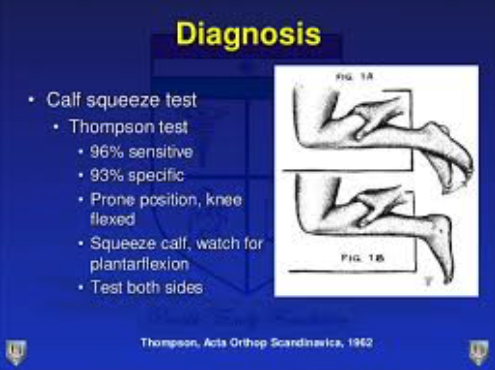 Simmonds’/Thomas calf squeeze test. Imaging is typically not necessary.
Simmonds’/Thomas calf squeeze test. Imaging is typically not necessary.
- An X-ray may be useful to confirm the presence of a calcification if the patient does not respond to a 6-month course of conservative treatment.
The rupture of the Achilles tendon requires an urgent referral to ER for appropriate splinting in plantar flexion or surgical intervention.
Treatment
Conservative treatment
Non-surgical treatment is recommended for at least 6 months before considering surgery. More than 90% of patients will get better with non-surgical treatment. Non-surgical treatment may consist of:
- Activity modification (decrease in high-impact activities such as running, and focus on cross-training activities such as biking, swimming, elliptical exercise)
- Icing
- NSAIDs or pain relief medication
- There is presently some research questioning whether NSAIDs slow the healing process of a tendinitis/tendinopathy condition
- Physiotherapy
- Physiotherapy treatment should typically address pain relief, activity modification, foot and gait analysis. The strengthening program should focus on eccentric loading exercises for the calf. Research shows that this type of exercise provides better outcomes by decreasing pain and improving function.
- Patients should beware of overstretching the structures as this may actually be a cause of the condition and/or perpetuate it.
- Heel lift
- Supportive shoes and possibly orthotics
Cortisone injections are not recommended due to possible tendon rupture.
Shock wave therapy may be recommended for a slow healing tendon or if there is a diagnosis of a calcification in the tendon as this treatment technique re-initiates the healing process.
Surgical treatment
Surgical treatment involves debridement of the scar tissue and calcification, and may involve a tendon transfer. After surgery, patients usually wear a cast, boot or brace for 6-8 weeks. Physiotherapy is recommended to assist in restoring strength, gait and function. Recovery can take 1-2 years.
Ankle sprain/chronic instability/fracture
Diagnosis
In case of a severe ankle sprain, a fracture should be excluded by use of the
Ottawa Ankle Rules (OAR). The OAR must be used within 1 week of the initial trauma for the tool to be valid and accurate.
When a grade 2 or 3 sprain is suspected, the result of an anterior drawer test is optimized when the clinical assessment is delayed for 4-5 days post-injury.
With persistent symptoms, an MRI may be requested to diagnose underlying joint damage but would be unnecessary to diagnose an uncomplicated rupture of the ATFL since a delayed physical assessment is sufficient.
Treatment
Care should be taken with prescription of NSAIDs after ankle sprain. They may be used to reduce pain and swelling for an acute sprain, but usage is not without complications and NSAIDs may suppress the natural healing process.
A topical NSAID (Voltaren Emulgel, Pensaid) can be suggested and has been proven effective in the literature.
Best practice guidelines indicate that cryotherapy in conjunction with exercise therapy has a greater effect on swelling and results in significant improvements in ankle function in the short term, allowing patients to increase loading during weight-bearing.
Use of a functional (lace-up or semi-rigid) support and exercise therapy provide better outcomes than immobilization. Use of a functional ankle support is recommended over a compression bandage. Bracing for 4-6 weeks is preferred over immobilization. If immobilization is applied to treat pain and edema it should be limited to a maximum of 10 days after which functional treatment should be initiated.
Exercise therapy, preferably in the form of supervised physiotherapy, should be initiated early following an acute sprain and consist of neuromuscular and proprioceptive exercises. This is shown to decrease the prevalence of recurrence and instability, leading to quicker recovery and better outcomes.
There is no evidence that RICE (Rest, Ice, Compression, and Elevation) alone is effective in the treatment of acute ankle sprains.
Surgical treatment
Surgical treatment is very rarely necessary to repair complete lateral ligament rupture. Surgical treatment may be preferred for professional athletes to ensure quicker return to play. ORIF surgeries are common to stabilize displaced ankle fractures.
https://www.ncbi.nlm.nih.gov/m/pubmed/29514819/