Arthritis
There are many types of arthritis, but primarily 3 that affect the knee joint:
- Rheumatoid arthritis: this occurs when the body’s immune system attacks healthy tissues including joints.
- Osteoarthritis: this is a “wear and tear” type of arthritis where the cartilage layer becomes thinner and thinner until the bones are touching – “bone on bone” – causing pain and stiffness of the joint. Osteoarthritis is associated with obesity and is thought to have a link with family history/genetics.
- Post-traumatic arthritis: this occurs after an injury to the knee.
Causes
There are several factors that may predispose someone to developing osteoarthritis in the knee:
Age and Genetics
It is normal for joints to change as we age and “wear down”. This is especially true in our weight-bearing joints such as our knees and hips. The ability of our cartilage to repair itself decreases as we age. Our genetics (family history) can predispose us to developing arthritis.
Weight
Our weight directly affects how much load our lower limb joints must carry during our everyday activities. It is also thought that obesity may cause inflammation that can damage our joints. Obesity is one of the most common risk factors for arthritis.
Previous Knee Injury
A previous knee injury may cause damage to the bone, the cartilage, meniscus or ligaments in your knee. This can then lead to abnormal loads on your knee joint in your everyday tasks
Symptoms
- Pain usually develops slowly over time
- Occurs especially in the morning or after sitting for a long period of time
- Swelling and heat in the joint
- Stiffness and a decreased range of motion of the knee
- Knee feels unstable -like it will buckle
- May lock or make snapping or clicking or grinding noises accompanied by pain.
Diagnosis
Knee arthritis is diagnosed by your doctor who will ask about your symptoms, do a physical examination and may confirm with a standing X-ray.
Treatment
It is possible to remain active and relatively pain-free despite a diagnosis of osteoarthritis. Many patients have minimal or no pain, despite having arthritis.
Conservative treatment should be tried first. This includes:
- Rest and/or activity modification
- Use of oral or topical (e.g. Voltaren emulgel cream) NSAIDs or pain relief medication (Tylenol/acetaminophen)
- Physiotherapy and exercises
- Weight loss
- Taping
- Heat/icing
- Shoe orthotics/supportive footwear
- Compression sleeve and/or unloader brace (which helps take weight off the affected compartment of the knee)
- Walking aid (cane, walker, crutches, walking poles)
- Cortisone injection
- Viscosupplementation
If your family doctor does not give injections, you may be referred to a sports medicine doctor.
Physiotherapy should focus on education, promotion of physical activity and general health. The physiotherapist will help you with pain control, knee range of motion, leg, hip, core and general strengthening exercises, assess your gait and balance and possibly suggest a walking aid if necessary. The therapist might introduce you to yoga or Tai chi as well as other exercise options such as swimming, aqua-fit and cycling, as well as a home exercise program.
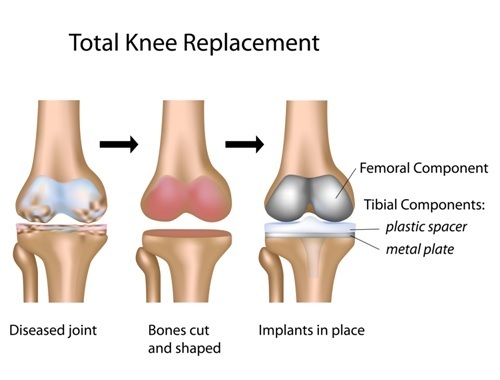 Surgical treatment is considered if the conservative measures do not help with pain and function of your knee. The surgery for arthritis is a partial or total knee replacement or occasionally an osteotomy (see below). These surgical procedures are highly successful for the treatment of pain from knee osteoarthritis. Knee surgery decreases pain, restores everyday function and generally leads to a better quality of life for people who suffer from advanced OA of the knee.
Surgical treatment is considered if the conservative measures do not help with pain and function of your knee. The surgery for arthritis is a partial or total knee replacement or occasionally an osteotomy (see below). These surgical procedures are highly successful for the treatment of pain from knee osteoarthritis. Knee surgery decreases pain, restores everyday function and generally leads to a better quality of life for people who suffer from advanced OA of the knee.
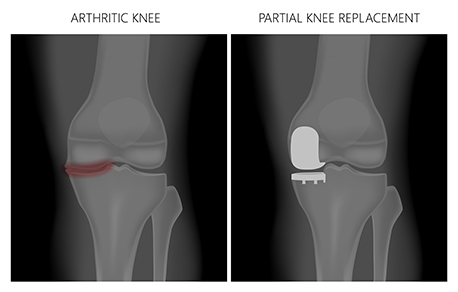
For a knee replacement, the bony surfaces of the joint are removed, and then metal pieces are inserted onto the end surfaces of the tibia and femur. A plastic lining in between the two new surfaces acts as the new cartilage. A plastic button is sometimes also placed behind the kneecap (patella) to allow for smooth movement. A partial knee replacement involves placing metal and plastic in one area of the knee only. A knee replacement typically lasts about 15 years. When or if it wears out, a revision may be necessary to remove the old metal pieces and reinsert a new the joint replacement.
An osteotomy is a procedure where the leg is broken and realigned to offload the damaged area. An osteotomy typically lasts 10-15 years at which time a knee replacement can be performed if necessary.
 After kneee surgery, you will start an outpatient rehab program which takes place at the hospital. You will take part in the rehab program in addition to doing daily exercises at home. Following joint replacement surgery, the program typically starts within 2-3 weeks after you are discharged from hospital. This is covered by OHIP. You may choose to seek treatment at a private clinic for your entire rehab program or complement what you are doing at the hospital with private physiotherapy. Each hospital has a different rehab schedule – please refer to the patient education booklet at your surgical site.
After kneee surgery, you will start an outpatient rehab program which takes place at the hospital. You will take part in the rehab program in addition to doing daily exercises at home. Following joint replacement surgery, the program typically starts within 2-3 weeks after you are discharged from hospital. This is covered by OHIP. You may choose to seek treatment at a private clinic for your entire rehab program or complement what you are doing at the hospital with private physiotherapy. Each hospital has a different rehab schedule – please refer to the patient education booklet at your surgical site.
Research shows that supervised rehabilitation by trained health professionals early after discharge optimizes outcomes.
Your physiotherapist will monitor your progress and work with you to recover your knee mobility, strength and balance, as well as help you restore your walking pattern, confidence on stairs, general function and fitness. You will also be provided with a comprehensive home exercise program. Typically, rehabilitation will take about 8-12 weeks with visits usually 2 times/week in the first few weeks. Some people require prolonged physiotherapy after knee surgery – please discuss with your treating physician and physiotherapist.
Anterior Cruciate Ligament (ACL) Injury
There are 3 bones in the knee joint: the femur (thigh bone), the tibia (shin bone) and the patella (kneecap). Bones are held together with ligaments and there are four ligaments in the knee. The medial collateral and the lateral collateral ligaments are on the sides of the knees and control the sideways motion of the knee. The anterior and posterior cruciate ligaments are inside the knee joint and form an “X”. They control the back and forth motion of the knee as well as knee rotation. The ACL is critical to the stability of your knee by controlling excessive motion of your knee. An injury or rupture to this ligament will likely affect your normal activities as well as your participation in sports.
Damage to a cruciate ligament often also results in damage to other structures in the knee like the cartilage (meniscus).
Ligament injuries are called sprains and are graded from 1 (least damage) to 3 (most damage). Grade 1 means that the ligament has been stretched, but it is still often able to stabilize the knee. Grade 2 means that the ligament has been stretched so it is loose or partially torn. Grade 3 is a complete tear of the ligament resulting in an unstable knee.
Cause
An ACL tear is usually a sports-related injury but can occur during any activity involving changing direction quickly, landing from a jump incorrectly or stopping suddenly. ACL tears can be caused by a direct collision or contact to the knee or leg.
Symptoms
- Temporary symptoms occur within seconds after injury and eventually go away after a few weeks with rest and physiotherapy.
- a “popping” noise with the injury
- severe pain and inability to continue with activity
- significant swelling and maybe bruising
- loss of range of motion in knee
- pain with walking
- Permanent symptoms – occur in the long term for some patients with a torn ACL
- knee feels unstable or “gives out” especially with twisting movements.
NOTE: pain is not a typical symptom of a torn ACL after the swelling and inflammation related to the initial injury has gone away. Most patients with a torn ACL have no pain in their knee – the knee simply feels wobbly or unstable.
Diagnosis
An ACL tear is diagnosed by taking a history and doing a physical examination of your knee which will include special tests of your ligaments. Most ligament injuries can be diagnosed by a physical exam. An X-ray may be ordered at the time of injury to make sure there are no associated fractures. An MRI may be done to confirm if the ACL is torn and it can confirm if there is damage to the cartilage as well.
Treatment
- Decision on whether knee surgery is necessary will depend on the functioning of your knee, your personal goals and progress with physiotherapy. Not all patients with ACL tears require surgery but rehabilitation is needed after most ACL injuries whether knee surgery is necessary or not.
- People who require knee surgery usually:
- Have completely torn their ACL or have a partial tear but a very unstable knee
- Have gone through a rehab program and the knee remains unstable
- Are very active in sports or have a physical job that requires knee stability (such as construction work, police work, firefighting, military work)
- Are willing to commit to a long and demanding rehabilitation program
- Have an unstable knee that affects their quality of life
- Have injured other structures in the knee (meniscus or cartilage, other ligaments)
It is possible that regular, progressive and guided rehabilitation can allow a person to resume high-level activities and “cope” with such an injury without having surgery.
Conservative treatment is often chosen when:
- There is a minor tear in the ACL.
- Your knee feels stable and doesn’t buckle or give out despite having a significant ACL tear (some patients have no knee instability despite having a completely torn ACL).
- Your lifestyle is not very active, and your work does not require a stable knee.
- You are willing to stop doing activities that require a stable knee (dancing, skiing, hockey).
- You can follow a rehab program that will help strengthen and stabilize your knee to reduce the chances of re-injury and are willing to live with a small amount of knee instability.
- You do not feel motivated to complete a long and demanding rehab process after knee surgery.
- You have medical problems that make having surgery risk.
Non-surgical treatment will usually involve physiotherapy and is most successful if therapy is initiated early (in the first 90 days) after ACL injury.
The rehabilitation program will have a goal of restoring your strength and function and should include some low-impact cardiovascular exercise (swimming, bicycle), range of motion exercises to gain as much movement of your knee as possible (it is especially important to regain the full straightening of your knee), strengthening exercises for your quadriceps, hamstrings, and gluteals, and balance training. If you are an athlete, the rehabilitation process will include sport specific preparation exercises. If your knee remains unstable despite rehabilitation, it might be necessary for you to wear a brace for activity.
Surgery is done in an attempt to restore the normal or almost normal stability in the knee and the level of function you had before the injury. It most often involves grafting a piece of your own patellar (kneecap) or hamstring tendon to replace the torn ACL ligament. This is done by an orthopedic surgeon through arthroscopic surgery – when small holes are made in the skin and tiny instruments are inserted in your knee to do the repairs. This surgery is done on an outpatient basis therefore you usually do not have to spend the night in the hospital.
After knee surgery, you may have a brace and crutches. ACL reconstruction surgery usually requires a commitment (6-12 months) to a rigorous rehabilitation and exercise program to improve your chances of successfully returning to a prior level of function.
It is
important to note that regardless of whether surgery is performed or not on an ACL injury, it is essential to regain FULL knee extension (straightening) after your injury. A knee that does not straighten fully will not function normally and will develop arthritis at an accelerated rate.
Meniscus Tears

The knee has two crescent-shaped cartilage pads which act as a shock absorber called menisci. They help to keep the knee stable and absorb some of the stresses from walking and weight-bearing. They are located between the thigh bone (femur) and the shin bone (tibia) that make up our knee joint. There is a medial (inside) and lateral (outside) meniscus.
Cause
The younger population tends to injure their meniscus by sudden trauma like a twisting motion with a slightly bent knee. This is often, but not always, a sport-related injury. In the older adult, a meniscal tear can result from natural age-related degeneration of the meniscus making it more vulnerable to tearing. This can often occur during daily activity. Degenerative tears can occur from a twisting motion, deep knee bending especially in a deep squat, or just from repetitive movements.
Symptoms
- “Popping” sound at time of injury
- Pain and swelling – will likely still be able to walk on the knee
- Inability to fully straighten or bend the knee – may feel locked
- Feeling of “locking” or “catching”
- Pain with twisting or squatting / deep bending movements of the knee.
Diagnosis
A meniscal tear is diagnosed by discussing your history and symptoms as well as a performing a physical examination consisting of some specific tests. X-rays do not show meniscus tears, but your doctor may order one to rule-out other causes of knee pain, such as arthritis. If you have arthritis, you likely also have meniscal tears. However, for a vast majority of patients, the arthritis and not the meniscal tear is responsible for their pain. If your X-rays show mild or no sign of arthritis your doctor may request an MRI to look for other causes of knee pain.
Treatment
Meniscus tears usually do not heal; however, the majority will stop hurting over time (6 months) and do not need surgery. A large meniscus tear may continue to hurt despite conservative treatment. Having a meniscus tear increases the risk of knee arthritis developing or progressing in the future.
Conservative treatment involves:
- Rest/activity modification
- Ice
- Physiotherapy
- NSAIDs (Advil/Ibuprofen) or pain relief medication (Tylenol/Acetaminophen)
Physiotherapy treatment will aim to decrease pain and swelling, improve joint range of motion, strengthen the muscles around your knee (quadriceps and hamstrings), strengthen the muscles around your hips and core, improve your balance and restore functional strength according to the activities and sports you practice. Recovery usually takes a few weeks but can take up to 6 months.
It is essential to regain full knee straightening (extension) and to
regain as much bending (flexion) as possible after your injury. Stiff
knees do not function normally and develop arthritis at an accelerated
rate.
Surgical treatment
Indications for surgical treatment of a torn meniscus include:
- A displaced meniscus tear especially if the displaced piece is blocking the knee from straightening or bending fully – this is called a “locked knee.” If you have a displaced meniscus tear which is interfering with knee motion, then knee surgery is usually performed within a few days to weeks in order to restore knee motion.
- Intermittent “locking” where the knee is temporarily unable to straighten or bend fully when the torn meniscus moves out of position. The knee “unlocks” when the piece moves back into correct position, however, it can “lock” again if the piece moves out of position in the future.
- Pain at the joint line corresponding to the meniscus tear despite an attempt at conservative treatment.
Knee surgery to address the meniscus tear is only performed after at least 6 months of conservative treatment (except for a locked knee – see above) with the understanding that knee pain may not improve. It is generally not considered if you have moderate to severe knee arthritis.
Surgical treatment of the meniscus is done by knee arthroscopy - when small holes are made in the skin and tiny instruments are inserted to clip (meniscectomy) or repair (meniscal repair) the meniscus.
The meniscectomy: During a meniscectomy, the torn meniscus fragment is removed. Healthy meniscus tissue is left alone. You will be allowed to put full weight on your leg and can increase your activity as tolerated. Recovery may take 4-8 weeks with return to sports being possible for most patients within 8 weeks after surgery.
Meniscus repair: Meniscus repair is less common than meniscectomy. Meniscus repair is only possible for some patients. When the surgeon repairs the meniscus, it is usually stitched and requires the torn meniscus fragment to heal in order to be successful. In order for the meniscus to heal the tear must be in the portion of the meniscus that has a good blood supply (outer 1/3) and the torn piece must be relatively undamaged. You may not be allowed to put weight on your leg for 4-8 weeks after a meniscus repair and may be asked to use a splint during this time. After a meniscus repair you will usually not be allowed to run, jump or do deep squats for 4 months. Return to sports is usually possible approximately 6 months following surgery.
Osteonecrosis/Avascular Necrosis of the Knee
Osteonecrosis occurs when the blood supply to the bones in the knee is disrupted. Without an adequate blood supply, the bone cannot repair itself and collapses. The cartilage also collapses, and this leads to arthritis. Osteonecrosis is more likely to occur in women and in those people over the age of 60.
Cause
- A prior injury
- Long term steroid medications (e.g.: Prednisone)
- Obesity
- Excessive alcohol use
- Medical conditions such as sickle cell anemia and lupus
Symptoms
- Pain can occur suddenly or after an injury
- Swelling and tenderness to touch
- Redness, warmth and redness
- Pain with weight-bearing, walking
- Decrease in the range of motion of the joint.
Diagnosis
Your doctor will discuss your history and symptoms, then carry out a physical examination. Your doctor will send you for an X-ray and possibly an MRI.
Treatment
The condition may cause pain for months. It is usually a slowly progressing disease. In some cases, the pain may stop without knee surgery over time.
Conservative treatment:
- Activity modification
- Pain relief medication (Tylenol, Acetaminophen)
- Decreased weight-bearing on the affected leg
- Physiotherapy/exercise
- Walking aid (crutches or cane)
Surgical treatment:
The surgical treatment for osteonecrosis of the knee is usually surgery to try to increase the blood supply or a knee replacement.
- Arthroscopy
- Young or very active patients may benefit from debridement of the necrotic region with removal of loose fragments and possibly drilling of the necrotic bone to stimulate blood flow.
- Arthroplasty
- Older patients with underlying osteoarthritis may benefit from a partial or total knee replacement
 The patello-femoral joint is where your patella (kneecap) glides over your thigh bone (femur). Your thigh bone has a groove (femoral groove) and your kneecap glides along this groove with knee movement. Both surfaces are lined with cartilage to make them smooth. Your quadriceps (thigh) muscle begins at the top of your thigh, runs over the kneecap and attaches just under the patella to the top of your shin by becoming the patellar tendon. Your quadriceps muscle has 4 parts to it. Two of the main parts of the quadriceps, the vastus lateralis (VL) and the vastus medialis oblique (VMO), make your patella track in its groove. The vastus lateralis pulls your kneecap up and outwards whereas the vastus medialis oblique is the only quadriceps muscle that pulls your kneecap up and slightly in.
The patello-femoral joint is where your patella (kneecap) glides over your thigh bone (femur). Your thigh bone has a groove (femoral groove) and your kneecap glides along this groove with knee movement. Both surfaces are lined with cartilage to make them smooth. Your quadriceps (thigh) muscle begins at the top of your thigh, runs over the kneecap and attaches just under the patella to the top of your shin by becoming the patellar tendon. Your quadriceps muscle has 4 parts to it. Two of the main parts of the quadriceps, the vastus lateralis (VL) and the vastus medialis oblique (VMO), make your patella track in its groove. The vastus lateralis pulls your kneecap up and outwards whereas the vastus medialis oblique is the only quadriceps muscle that pulls your kneecap up and slightly in.
Patello-femoral Pain Syndrome is the medical term for pain felt behind your kneecap, at the patello-femoral joint. It is a common condition that affects 25 % of the population at some time in their life. Patello-femoral Pain Syndrome commonly affects teenagers, active individuals, runners, adults who sit for a living and people who have recently increased their level of activity.
Cause
The exact cause of patello-femoral pain syndrome is not clear. It may be due to excessive pressure under the patello-femoral joint from poor kneecap alignment which may cause irritation. Bending your knee automatically increases the pressure behind your kneecap. This can cause irritation and thinning of the patello-femoral cartilage over time. A muscle imbalance between parts of your quadriceps muscle (the vastus lateralis - VL and the vastus medialis -VMO) causes poor tracking of the kneecap. Often the VMO is not strong enough to counter the pull of the VL or to overcome the tightness of your lateral (outside) knee structures (lateral retinaculum, VL, and ITB). This will cause your kneecap to track outwards.
Other contributing factors to poor kneecap tracking are poor foot mechanics (flat feet) and weak hip and buttock and core muscles.
Symptoms
- Comes on gradually - no injury
- May be felt at rest - especially if your knee is bent for a long time
- Worse with stairs, hills, walking, squatting, kneeling, running or jumping
- Aggravated by wearing high heel shoes
- Aggravated by exercising on an inclined treadmill
Diagnosis
Your doctor can diagnose this condition by discussing your history and symptoms with you and doing a physical examination of your knee. X-rays are usually unnecessary.
Treatment
Most people will recover with:
- Rest and/or activity modification
- it is essential not to “push through” patellar pain
- aggravating exercises and activities should be stopped until the pain improves and restarted gradually
- Non-aggravating aerobic exercises can be helpful
- if stationary biking is painful try an elliptical machine – it may feel better because there is less knee bending required.
- Icing
- Oral (Advil/Ibuprofen) or topical (e.g. Voltaren emulgel) NSAIDs or pain relief medication (Tylenol/Acetaminophen)
- Patellar tracking brace or taping (McConnell taping) may help
- Physiotherapy
- Custom orthotics or good quality store-bought supportive insoles (e.g. Superfeet)
- Avoiding flip flops
Physiotherapy is very effective in treating patello-femoral pain; 90% of PFS sufferers will improve within 6 weeks of starting a physiotherapy-guided rehabilitation program.
Physiotherapy treatment will likely focus on pain control, education, gait analysis, knee range of motion, balance, stretching and specific strengthening exercises for your hip, glute, core and quadriceps (especially your VMO).
Knee surgery is rarely necessary. However, it may be required in certain cases
- persistent pain despite a prolonged trial of non-operative treatment AND improvement in symptoms when the patella is pulled inwardly with taping (McConnell taping)
- severe patello-femoral arthritis