Subacromial Bursitis
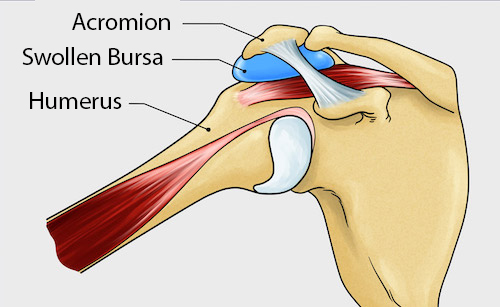 Subacromial bursitis is caused by an impingement of the bursa between the rotator cuff tendons and the bony cap (acromion) of your shoulder. Bursae are small, fluid-filled sacs located near joints, like the shoulder. They function like cushions to reduce friction with the gliding motion between the bone and the soft tissue or muscles.
Subacromial bursitis is caused by an impingement of the bursa between the rotator cuff tendons and the bony cap (acromion) of your shoulder. Bursae are small, fluid-filled sacs located near joints, like the shoulder. They function like cushions to reduce friction with the gliding motion between the bone and the soft tissue or muscles.
Cause
Sometimes, if your shoulder has abnormal mechanics, excessive or altered motion, this will cause the bursa to become irritated and swell. It will then get pinched, especially with shoulder movements that involve lifting your arm to the side. A trauma like a fall onto your shoulder may also be a cause.
The subacromial bursa is the most commonly inflamed of the shoulder bursae. It is often present with rotator cuff tears or tendinitis (see below). These two conditions frequently re-occur if you return to activity too quickly, especially without completing a thorough rehabilitation program.
Calcific bursitis occurs when a shoulder bursitis is neglected, when the inflammation becomes chronic or when the healing process goes wrong. Bone (calcium deposit) growth occurs in the bursa over time and the symptoms become chronic.
Symptoms
- Pain in the shoulder that begins gradually or very suddenly located on the outside of your shoulder and possibly spreading down your arm
- Increased pain with lying on the painful shoulder or when the arm is above your head
- Painful arc of movement – shoulder pain at 60-90 degrees when moving the arm up and outward
- Pain with activities that require reaching forward or back
- Weakness in the arm
Diagnosis
Your doctor will discuss your history and symptoms, then proceed to a physical examination.
She or he may send you for X-rays (to rule-out any issues with the bones in your joint), an ultrasound (to show the soft tissues and muscles around your shoulder, as well as calcium deposit if there is some), or an MRI (to rule-out a rotator cuff tear or to determine if shoulder surgery is considered). In most cases an MRI is not necessary unless there is no improvement with conservative treatment.
Treatment
This condition is unlikely to need shoulder surgery. Treatment includes:
- Rest and/or activity modification
- Ice (20 min, 2-3 times/day)
- Oral (Advil/Ibuprofen) or topical (e.g. Voltaren emulgel) NSAIDs or pain relief (Tylenol/Acetaminophen) medication
- Physiotherapy
- Taping
- Cortisone injection to help reduce the inflammation
Your doctor may refer you to a sports medicine doctor for an injection. It sometimes is performed under ultrasound guidance.
Research has proven that physiotherapy will help you to recover quicker and reduces the likelihood of recurrence.
Physiotherapy will initially focus on pain relief and gentle shoulder range of motion exercises. Once your pain subsides, it becomes important to properly strengthen the rotator cuff muscles because they are the ones that control and stabilize your shoulder, ensuring the ball remains centered as it glides in its socket. This prevents structures (bursae and tendons) in your shoulder from becoming pinched when you move your arm. The rehabilitation program should also include exercises to improve the strength and motor control of the muscles around your shoulder blade. The physiotherapist might also direct some treatment at your neck and upper back to help improve your shoulder movement and posture. Depending on your lifestyle or the sports you practice, your physiotherapist will guide you through some functional exercises that prepare you to return to your activities.
Typically, rehabilitation will take 6-12 weeks, but can extend up to 6 months.
If calcific bursitis is diagnosed your doctor might suggest shock wave therapy as this treatment re-initiates a healing process. It should be followed-up with a physiotherapist-guided rehabilitation program.
Rotator Cuff Syndrome (Shoulder Impingement/Rotator Cuff Tendinitis and Tendinopathy)
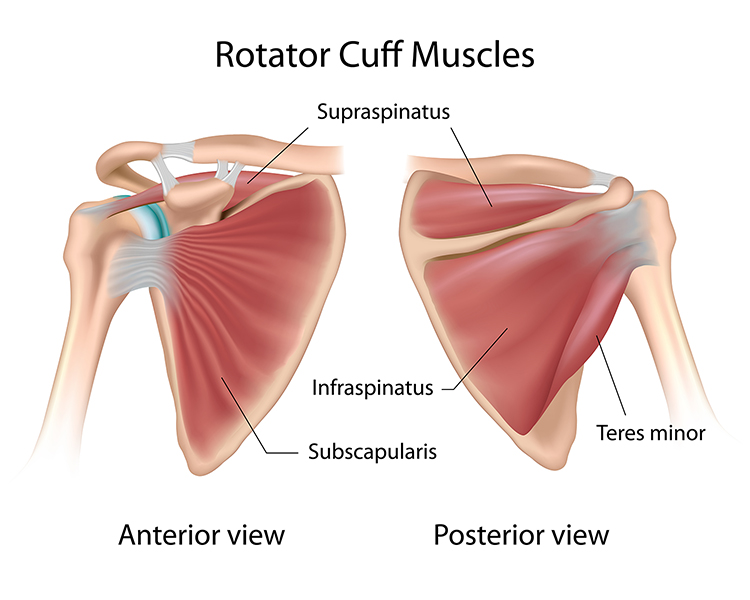
The rotator cuff is a group of four muscles and their tendons (supraspinatus, infraspinatus, subscapularis and teres minor) that surround the shoulder to provide it with movement and stability. The rotator cuff tendons originate from various points on the shoulder blade and attach to the humerus, creating a cuff over the shoulder. Its functions are to lift and move the shoulder, as well as to keep the ball centered and stable in its socket. The shoulder bursa is also in this area (
see bursitis above) and can become inflamed when the rotator cuff is injured or torn. Rotator cuff pain can be caused by:
- Bursitis (explained above)
- Tendinitis/tendinosis
- When one or more of the rotator cuff tendons become inflamed or injured
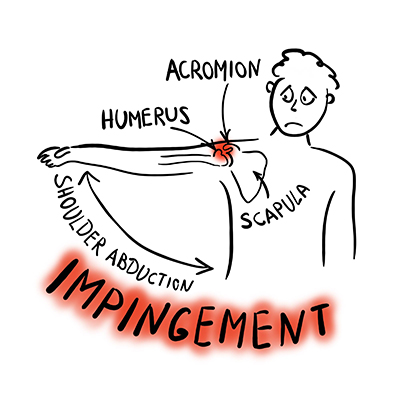
- Impingement: This is when the structures (bursa and/or rotator cuff muscle tendons) become pinched in the space between the acromion and the ball (head of the humerus) as you move your arm. This happens most often to the supraspinatus tendon because of its position
- A tear in one of the four rotator cuff muscles (see rotator cuff tear below)
Causes of shoulder impingement and rotator cuff tendinitis can be:
 A minor injury
A minor injury - Repetitive motions such as lifting and reaching overhead
- Demands that exceed what your muscle can handle; therefore, it becomes injured
- Abnormal mechanics, excessive or altered motion
- A trauma - like a fall
- Poor posture
Symptoms
- Pain on the outside of the shoulder and upper arm
- Pain at night
- Pain at rest
- Pain and/or clicking when moving your arm – especially at certain angles like when lifting it out to the side, over your head or behind your back
- Loss of strength
- Loss of range of motion
- Worse with activity
Diagnosis
Your doctor will ask about your history and symptoms then carry out a physical examination. He or she may send you for X-rays (to rule-out any issues with the bones in your joint), an ultrasound (to show the soft tissues and muscles around your shoulder, as well as calcium deposits if there are some), or an MRI (to rule-out a rotator cuff tear or to determine if shoulder surgery is needed). In most cases an MRI is not necessary unless there is no improvement with conservative treatment.
Treatment
Most patients do not need shoulder surgery because shoulder tendinitis is reversible and successfully treated with conservative measures.
It may take 3-6 months for symptoms to subside
Conservative measures include:
- Rest and/or activity modification (limit overhead or painful activities)
- Ice/heat (alternating can be helpful)
- Oral (Advil/Ibuprofen) or topical (e.g. Voltaren emulgel) NSAID or pain relief (Tylenol/Acetaminophen) medication – However, recent research indicates the possibility that NSAIDs may slow down the healing process in muscle injuries. You can discuss with your family physician.
- Physiotherapy
- Taping
- Cortisone injection
- If your family doctor does not give injections, you may be referred to a sports medicine doctor
Research has proven that physiotherapy will help you recover more quickly and reduces the likelihood of recurrence.
Physiotherapy will initially focus on pain relief and gentle shoulder range of motion exercises. Once your pain subsides it becomes important to properly strengthen the rotator cuff muscles because they are the ones that control and stabilize your shoulder, ensuring the ball remains centered as it glides in its socket. This prevents structures (bursae and tendons) in your shoulder from becoming pinched when you move your arm. The rehabilitation program should also include exercises to improve the strength and motor control of the muscles around your shoulder blade. The physiotherapist might also direct some treatment at your neck and upper back to help improve your shoulder movement and posture. Depending on your lifestyle or the sports you practice, your physiotherapist will guide you through some functional exercises that prepare you to return to your activities.
Typically, rehabilitation will take 6-12 weeks but can extend up to 6 months.
Surgical treatment is considered only if the conservative measures are not helpful. The type of shoulder surgery will depend on your condition but may be arthroscopic (using small instruments inserted through small holes in your shoulder) or through a larger incision. After surgery, you will likely wear a sling temporarily and will have physiotherapy to help you improve strength, range of motion and function.
Rotator Cuff Tear
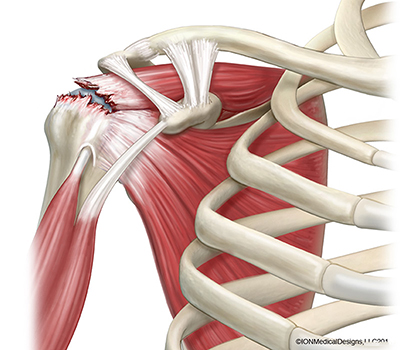 The rotator cuff is a group of four muscles and their tendons (supraspinatus, infraspinatus, subscapularis and teres minor) that surround the shoulder to provide it with movement and stability. The rotator cuff tendons originate from various points on the shoulder blade and attach to the humerus creating a cuff over the shoulder. Its functions are to lift and move the shoulder as well as keep the ball centered and stable in its socket. The subacromial bursa is also in this area (see bursitis above) and can become inflamed when the rotator cuff is injured or torn.
The rotator cuff is a group of four muscles and their tendons (supraspinatus, infraspinatus, subscapularis and teres minor) that surround the shoulder to provide it with movement and stability. The rotator cuff tendons originate from various points on the shoulder blade and attach to the humerus creating a cuff over the shoulder. Its functions are to lift and move the shoulder as well as keep the ball centered and stable in its socket. The subacromial bursa is also in this area (see bursitis above) and can become inflamed when the rotator cuff is injured or torn.
A rotator cuff tear is a tear to one or more of the rotator cuff tendons or muscles.
Cause
A rotator cuff tear can occur from an acute injury/trauma, or it can fray due to repeated trauma (overuse) or degeneration over time. You can have a partial tear or a full-thickness tear. An acute tear will likely be caused from an injury like falling on an outstretched arm.
Research has shown that there are many people (17-23%) with degenerative rotator cuff tears confirmed on imaging who have no symptoms at all.
Symptoms
The degree of shoulder pain and weakness will increase with the severity of the rotator cuff tear.
Partial tear:
- Mild shoulder pain – especially when raising your arm or with reaching your arm behind your back
- Clicking or catching when raising arm
- Mild shoulder weakness
- Pain with activity
Full-thickness tear:
- Acute pain – especially at time of injury
- There may be a snapping sensation on injury
- Pain at night – difficulty sleeping
- Marked weakness - inability to raise the arm, noticeably decreasing its function
- Significant weakness with little or no pain – in some instances when the tear is severe
Diagnosis
Your doctor will ask about your history and symptoms, then he/she will do a physical examination of your shoulder.
An X-ray does not show a tear but may be used to rule-out arthritis. Diagnostic ultrasound and MRI are both accurate tests for diagnosing this condition. However, your family doctor will send you for an ultrasound first because it is less costly and has shorter wait time. An MRI is not likely necessary unless conservative treatment is not successful.
Treatment
Conservative Treatment:
About 80% of patients with partial rotator cuff tears get better with conservative management that may include:
- 3- 6 months of activity modification
- Ice/heat
- Oral (Advil/Ibuprofen) or topical (e.g. Voltaren emulgel) NSAID and/or pain relief (Tylenol/Acetaminophen) medication
- Physiotherapy
- Cortisone injection
- If your family doctor does not give injections, you may be referred to a sports medicine doctor
Physiotherapy should include daily postural and shoulder range of motion/stretching exercises. Rotator cuff strengthening exercises and shoulder blade exercises that focus on normalizing shoulder function and motor control. Rehabilitation can typically take 6 months.
Surgical treatment:
Large or full-thickness rotator cuff tears require shoulder surgery quickly and research shows that the best results are when surgery occurs within the first 6-12 weeks following the injury. Delay will make the surgical repair difficult and reduce the likelihood of a successful outcome because the rotator cuff tendon retracts and atrophies after injury.
Shoulder surgery may also be done for patients with persistent pain and weakness despite a trial (12 weeks minimum) of conservative treatment.
This may be done by arthroscopy (using small instruments inserted through a hole in your shoulder) or through a larger incision. After surgery, the shoulder would typically be immobilized for a period of 6 weeks and then you will require physiotherapy to help restore range of motion and strength, and to improve function. Full recovery usually takes 6 months.
Shoulder Instability/Dislocation
Shoulder instability/dislocation occurs when the head of the humerus (upper arm bone) is loose (instability) or gets pushed out of the socket (dislocation).
This usually occurs from repetitive motion (instability) or a traumatic injury (dislocation). When the upper arm bone comes partially out of the socket, it is called a subluxation. In a dislocation, it comes completely out of the socket. Some people have repeated dislocations of the shoulder, which cause the tendons and ligaments to become stretched, causing chronic shoulder instability.
Dislocation
Shoulder dislocation is a traumatic injury that causes instant, intense pain in the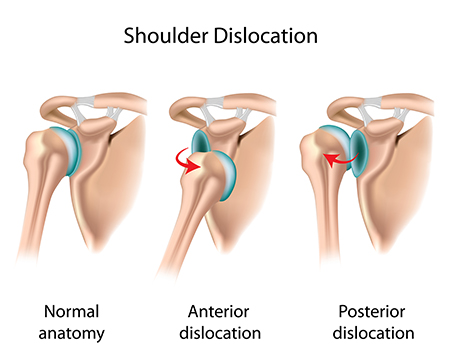 shoulder. The ball comes all the way out of the socket often tearing and/or stretching the ligaments, tendons and muscles around the shoulder.
shoulder. The ball comes all the way out of the socket often tearing and/or stretching the ligaments, tendons and muscles around the shoulder.
When this happens, you need to go to a hospital Emergency Room, where the doctor will help your shoulder slip back into the socket.
Following this, you might be immobilized in a sling for about 1-2 weeks, and early physiotherapy to recover your shoulder function with some range of motion and strengthening exercises. A physiotherapist can help guide your rehabilitation to help reduce the likelihood of a recurrence.
Unfortunately, once a shoulder has dislocated, it is vulnerable to repeat episodes, especially in younger people.
Instability
An injury or trauma may cause the shoulder to dislocate. If you have a severe first dislocation, it can lead to ligament or tendon damage which can cause the shoulder to become unstable. Some people who practice certain sports or activities such as swimming, baseball, or lifting may experience a repetitive strain that can cause the shoulder ligaments to become loose leading to chronic shoulder instability. This happens when the ligaments, tendons and muscles cannot keep the ball centered in its socket. Some people are born with naturally loose ligaments and the shoulder ball can come out of the socket in every direction that the shoulder moves.
Symptoms
- Pain in the shoulder
- Repeated dislocations
- A feeling that the shoulder is “loose” or “slips out”
- Catching or giving out
- Lack of confidence feel in moving the shoulder in some directions
Diagnosis
Your doctor will discuss your history and symptoms with you, then will do a physical examination of your shoulder. He or she will likely do some special tests to assess for instability in your shoulder. You may be sent for X-rays (to rule-out any issues with the bones in your joint) or an MRI (to properly see the soft tissues around your shoulder)
Treatment
Conservative treatment is attempted for several months before consulting with a surgeon. This includes:
- Rest and/or activity modification
- Oral (Advil/Ibuprofen) or topical (e.g. Voltaren emulgel) NSAIDs and /or pain relief (Tylenol/Acetaminophen) medication
- Physiotherapy
Physiotherapy will initially focus on pain relief and gentle shoulder range of motion exercise. Once your pain subsides it becomes important to properly strengthen the rotator cuff muscles because they are the ones that control and stabilize your shoulder, ensuring the ball remains centered as it glides in its socket. The rehabilitation program should also include exercises to improve the strength and motor control of the muscles around your shoulder blade. The physiotherapist might also direct some treatment at your neck and upper back to help improve your shoulder movement and posture. Depending on your lifestyle or the sports you practice, your physiotherapist will guide you through some functional exercises that prepare you to return to your activities.
Typically, rehabilitation will take 8-12 weeks but can be longer.
Surgical treatment is considered only if the conservative measures are not helpful. The goal is to repair and tighten up loose or torn ligaments or tendons so they can hold the shoulder in place.
The type of shoulder surgery will depend on your condition but may be arthroscopic (using small instruments inserted through a hole in your shoulder) or through a larger incision.
After surgery, you will likely be wearing a sling temporarily followed by physiotherapy to restore range of motion, strengthen and improve muscle function of your shoulder and shoulder blade muscles.
Arthritis
 There are many types of arthritis that can cause shoulder pain and loss of function, but there are three main ones:
There are many types of arthritis that can cause shoulder pain and loss of function, but there are three main ones:
1. Osteoarthritis
of the shoulder is a gradual loss of the cartilage in the shoulder
joint which then causes erosion of bony surfaces, pain and decreased
function. It generally occurs in people over 50 years of age.
Some causes of osteoarthritis include:
- Repetitive arm movements at work or with sport activities
- A prior injury to the shoulder
- Obesity – causes higher than normal levels of inflammation in the body which affects the cartilage
- Genetic predisposition
- Chronic
rotator cuff tear or shoulder instability which causes poor shoulder
mechanics which can cause or accelerate arthritic changes
2. Rheumatoid
arthritis is an autoimmune disease where the immune system attacks the
joints. It causes the lining of the joint to become swollen, inflamed,
and painful as the cartilage breaks down.
3. Post-traumatic arthritis is caused by a prior injury to the shoulder like a fracture or a dislocation.
4. Avascular
necrosis (AVN) is caused by a disruption of blood supply to the head of
the humerus. When bone cells lose blood supply, they die, causing a
collapse of the bone and a wearing down of the cartilage, resulting in
arthritis.
Some causes of Avascular necrosis (AVN) include:
- Heavy steroid use
- Heavy alcohol consumption
- Sickle cell disease
- Trauma to the shoulder
Symptoms
- Pain behind the shoulder and deep inside the joint – that becomes worse over time
- Pain at night
- Weakness
- Increased pain with overhead activities
- Stiffness and reduced range of motion
- Decreasing function of the shoulder (most noticeably with lifting arm overhead and turning it outward)
- Difficulty sleeping because of pain
- Grinding sounds with movement
Diagnosis
Your
doctor will discuss your history and symptoms as well as do a physical
examination or your shoulder. X-rays confirm an osteoarthritis
diagnosis. An MRI is not necessary.
Treatment
Conservative treatment is always tried first to help with pain and function.
Conservative measures include:
- Rest and/or activity modification
- Heat/ice
- Oral (Advil/Ibuprofen) or topical (e.g. Voltaren emulgel) NSAIDs or pain relief (Tylenol/Acetaminophen) medication
- Physiotherapy
- Cortisone injection
- If your family doctor does not give injections, you may be referred to a sports medicine doctor
Physiotherapy
will consist of education, general fitness, shoulder range of motion
and stretching exercises, strengthening exercises for the rotator cuff
and shoulder blade muscles. The physiotherapist might also direct some
treatment at your neck and upper back to help improve your shoulder
movement and posture. Because arthritis in your shoulder cannot be cured
it is important to maintain movement and strength in your shoulder
therefore the physiotherapist will likely recommend you keep up some
type of physical activity such as aqua-fit, tai-chi, exercise class
and/or a home exercise program.
Surgical treatment
The decision to do shoulder surgery often depends on your age and quality of life.
Partial
or total shoulder joint replacement surgery, where metal and plastic
parts are used to replace the worn-out joint is done to relieve pain and
improve quality of life when conservative treatments have been
exhausted.
Labral Tear
The labrum is a fibrous cartilage cup that lines the outside rim of the shoulder socket on your scapula (shoulder blade). It surrounds the socket to help make it 50% deeper, stabilizes the joint and serves as an anchor site for the biceps tendon and several ligaments.
Causes
- Trauma or prior injury - dislocation, falling on an outstretched arm
- A violent pulling or a reaching movement
- Repetitive overhead shoulder motion -throwing athletes
Symptoms
A labral tear is sometimes challenging to diagnose because its symptoms resemble those of many other shoulder injuries.
Symptoms may include:
- A feeling of instability in the shoulder
- Catching, locking, grinding with certain movements
- Pain with overhead activity
- Pain at night or with activity
- Decreased range of motion
- Loss of strength
Diagnosis
To diagnose a labral tear, your doctor will discuss your history, ask about your symptoms and carry out a physical examination that includes special apprehension tests. An X-ray might be requested to rule-out any bony joint causes. A tear is best diagnosed with the help of an MRI arthrogram. In this test, contrast dye is injected into the joint before taking the MRI. That way, if there are any flaws in the labrum, they can be seen more clearly.
Treatment
A conservative approach will often be effective in relieving the symptoms. This might include:
- Rest/activity modification
- Ice
- NSAIDs (Advil/Ibuprofen) or pain relief (Tylenol/Acetaminophen) medication
- Physiotherapy
Physiotherapy will focus on exercises to strengthen the muscles of your rotator cuff and shoulder blade, improve motor control of your shoulder, and improve posture.
Surgical treatment may be considered if conservative treatment has not succeeded in relieving your symptoms.
Shoulder surgery is most often done by arthroscopic surgery, where small incisions are made to allow instruments to be inserted to examine the rim and either remove a torn piece of labrum and/or repair an affected tendon or ligament in the shoulder joint. Occasionally the surgeon will choose to use a small incision on the front of the shoulder to do this surgery.
Post-surgery you will need to wear a sling for approximately 3-6 weeks. Once the sling is removed, you will need to begin to rehabilitate the shoulder movement and strength.
A physiotherapist can guide you with exercises to increase your range of motion and strength, as well as work with you to regain a functional motor control of your shoulder. A rehab program will last 8-12 weeks, although the shoulder can take 4-6 months to fully heal.
Adhesive Capsulitis/Frozen Shoulder

Frozen shoulder is also known as Adhesive Capsulitis. It is a very painful condition which severely limits your shoulder movement and function for 1 to 24 months.
It typically affects people in their mid-50’s and is slightly more common in women than men.
Cause
The actual cause is not really understood but it is generally believed that it is a result of inflammation and swelling of the lining of the shoulder joint called the capsule which then results in a painful and significant “tightening” of the joint.
There are two types of presentation:
- Idiopathic (“primary”) frozen shoulder occurs spontaneously without a specific injury or event. It is believed that it stems from an abnormal chronic inflammatory response by the immune system.
- Secondary adhesive capsulitis occurs following a shoulder injury/trauma or surgery, or may be happen with another condition such as diabetes, stroke, or cardiovascular disease. This type may take longer to recover and recovery might be less successful.
Symptoms
Frozen shoulder typically progresses in three overlapping phases:
- Phase 1 (months 2 to 9): The painful freezing phase is when the shoulder progressively loses range of motion and becomes increasingly painful with movement. It may be worse at night.
- Phase 2 (months 4 to 12): During the adhesive phase there is a gradual decrease in pain while stiffness remains and significant restrictions to range of motion set in.
- Phase 3 (months 12 to 42): The resolution phase is characterized by a gradual improvement in the range of motion of your shoulder and pain is only felt at the end limit of your shoulder movement.
Some people never recover all of their shoulder movement.
Diagnosis
Your family doctor will recognize frozen shoulder by listening to your history and symptoms, and by examining your shoulder movements.
Blood tests, X-rays and/or ultrasound usually are not required unless other conditions need to be ruled-out. X-ray can be useful to look for arthritis which is a common cause of shoulder stiffness.
Treatment
Conservative treatment is the first approach and may vary according to what stage you are in and how you respond:
- NSAIDs (Advil/Ibuprofen) or pain relief (Tylenol/Acetaminophen) medication
- Using your arm as much as possible to encourage movement
- Physiotherapy
- Cortisone injection
- Should your pain be constant and difficult to manage, your family doctor might recommend a cortisone injection. However, it is important to note that cortisone injection is useful to improve pain on the short term, but it does not shorten the natural course of the condition or recovery time
- If your family doctor does not give injections, you may be referred to a sports medicine doctor.
Physiotherapy will focus on teaching you some mobility and stretching exercises for your shoulder and will provide you with an important home exercise program. Rehabilitation will often take from 3 months to 1 year.
When you come out of phase 1, the painful freezing phase, you are encouraged to exercise the shoulder to increase its range of motion.
It is important to understand that frozen shoulder causes pain with all movements and that this pain is not harmful. Helpful exercises will involve gently coaxing your shoulder to repeatedly move into painful angles. When done properly, you will notice that it is painful to reach end-range of movement but when you come away the pain will immediately subside and even disappear.
Surgical treatment is generally not necessary for frozen shoulder. However, capsular release is a surgical procedure under general or regional anesthesia during which the contracted tissue is released. It is typically done by arthroscopy.
Avascular necrosis
Avascular necrosis (AVN) is a condition caused by a disruption of blood supply to the head of the humerus. When bone cells lose blood supply, they die which causes a collapse of the bone and a wearing of the cartilage resulting in arthritis.
Cause
- Heavy steroid medication use
- Heavy alcohol consumption
- Family history
- Blood disorders and disease (e.g.: Sickle cell disease, coagulation problems)
- Trauma to the shoulder (e.g.: shoulder dislocation)
Diagnosis
Your doctor will discuss your history and symptoms as well as do a physical examination or your shoulder. X-rays and MRI of your shoulder will be required to diagnose this condition.
Your doctor may check other joints for sign of similar problems. In some patients, osteonecrosis can also affect their hip, knee, ankle, wrist and/or elbow.
Symptoms
- Onset of pain can be slow and intermittent but eventually progresses to constant pain that travels to your elbow
- Deep throbbing pain in shoulder
- Locking in the joint (later stages)
- Stiffness and loss of movement
- Grinding feeling in shoulder with movement
- Weakness
- Pain at night – difficulty sleeping
Treatment
Conservative treatment- Rest and/or activity modification
- Medications to treat the underlying cause
- Pain relief medication (Tylenol, Acetaminophen)
- Stop consuming alcohol and tobacco products
- If on steroid medication – review need vs risk with prescribing physician
- Physiotherapy
- Range of motion exercises and some gentle strengthening
- Avoid overhead movements and lifting
Surgical treatmentIf conservative treatment is not helpful in providing pain relief and improving function, surgical treatment will involve arthroscopic debridement and/or core decompression to increase blood flow and clear the shoulder of any debris, if diagnosed early.
Arthroscopic debridement is done to remove loose bits of cartilage or bone and smooth the surface of the joint by inserting a tiny camera and instruments through small incisions in your shoulder.
Core decompression is done by drilling holes in the affected areas of bone to allow new blood vessels to grow in the area. The surgeon uses a special type of X-ray called fluoroscopy to guide Them.They may also remove some of the dead bone to cause bleeding which will help grow new bone.
In the mild to moderate stage of the disease the surgeon may decide to do a bone graft. This is when donor bone (usually from your own hip) is used to replace some of the dead bone with healthy bone and give it some support to help it heal.
In advanced stages of the disease
total or partial shoulder replacement will be the course of action.